

Unicompartmental knee replacements are made of metal, and often an alloy of cobalt-chrome or titanium is being used. In between the upper and lower leg components a plastic insert is placed, which is made of poly-ethylene. This poly-ethylene plastic is a very strong material that will only be susceptible to minimal wear with normal use.
A large proportion of patients with unicompartmental knee replacements is able to perform kneeling activities, but some discomfort can still be experienced around the kneecap during heavy loading or deep flexion. Work on the knees or peak loading of the kneecap (during long distance running for example) is not advised though due to higher risk of wear or loosening.
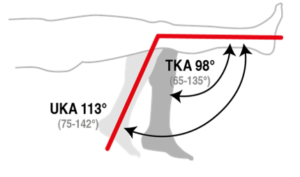
Normal activities in daily life such as walking, stair climbing, biking, swimming, fitness and gardening should be a realistic goal for most people after unicompartmental knee replacement. In comparison with total knee replacement approximately 10 to 15 degrees more flexion can be expected after rehabilitation of uni knee replacement.